Macular Degeneration Overview

Just to put things into perspective, by 2030s, for the first time in the history of the United States:
- All baby boomers will be older than age 65, i.e. 78.0 million people 65 years and older compared to 76.4 million under the age of 18. (Source)
And by 2050s,
- One fifth of the total U.S. population will be 65 or older, up from 12% in 2000 and 8% in 1950.
Of all other things, this also means a significant increase in the percentage of people susceptible to macular degeneration, or age-related macular degeneration (AMD or ARMD), as it is referred to otherwise. According to research; age-related macular degeneration is the biggest cause of irreversible vision loss in seniors.

It is a painless and irreversible degenerative eye disease that targets and damages the central part of the retina within the eye, the macula, which serves to help us view fine details clearly.
Since macular degeneration impairs central vision of a person, people suffering from it are troubled in performing tasks requiring clear central vision, such as reading, writing, threading a needle and so forth.
Due to macular function issues, experiencing blurriness or darkness in center of vision is a common outcome for AMD patients, though the peripheral vision remains unaffected, quite unlike what many people tend to believe somehow.
Age related macular degeneration is classified into two major types broadly, dry and wet.

While dry AMD cases outnumber wet AMD, the later one far outweighs the former in intensity and severity, capable of inflicting rapid and sudden loss of central vision.
Various elements considered helpful in treatment, in addition to different types of therapies and medication, also include dietary constituents and lifestyle changes aimed at halting the progression of age related macular degeneration. Early identification of this degenerative disease in patients with higher risk factor for it is also equally important.
Primarily affecting people above 65, some macular complications also target younger people, but generally, it is referred as “age related macular degeneration”. Macula, the sensitive region of the retina used for sharp central vision, is affected in this particular eye condition. As of now, despite the availability of various treatments for AMD, no certain cure exists for it.
What is Retina?
Located at the back of your eye, it comprises of the collection of light sensitive tissues, which serve to capture the images we see and pass them on to the brain via the optic nerve, after converting them into electrical impulses with the help of a chemical reaction. This conversion is almost instant and the resultant impulses or signals are passed on to the brain, which interprets all the visual information for us as the images we see.
What is Macula?
The small portion of the retina right at its center is referred as the macula, which helps you in seeing straight ahead (central vision) and identifying the finer details through your direct line of sight. Activities like reading, driving, color and face recognition are possible due to the macula. The remaining ‘non-macular’ region of the retina takes care of your side vision and night vision.
What is AMD/ARMD?
The group of eye disorders affecting the central region of the retina (thus affecting the central field of vision) is referred collectively as “macular degeneration”. Since people over 65 years of age serve as the prime target zone for this disease, ARMD happens to be the biggest single factor behind legal blindness in developed nations of the world.
According to a research:

And this high prevalence of age related macular degeneration impacts the U.S. in another aspect as well, i.e. the financial one:
Three different layers of tissues line the eye from the inside, each serving with distinct but critical functions for normal vision. “Retina” is the innermost layer, one which is struck first by the light rays entering the eye, comprised of a complex network of nervous tissues including the photoreceptor cells. Light is converted into electrical signals with the help of these photoreceptor cells and then processed and amplified by other types of cells, finally passing them on to the brain through the optic nerve.
“Macula” constitutes the central region of the retina, having a number of specialized structural features capable of enhancing the resolution of the images being focused on to it. Then there is the “Retinal Pigment Epithelium” layer (RPE), the single-cell-thick sheet constituting the middle layer. It not only offers metabolic support for the photoreceptor cells, but also manages the removal of cellular debris which is generated as a result of renewal of the photoreceptor cells.
The last layer constituting the retina comprises of a generous network of blood vessels, collectively referred as the “choroid”. RPE and photoreceptor cells get their share of oxygen and nutrients through these vessels, also carrying the waste products away.
One of the consequences of macular degeneration is the formation and accumulation of clumps of yellowish cellular debris (believed to be of retinal origin) behind the RPE. Initially, these deposits are not visible to the naked eye. These can only be observed by clinicians and optometrists taking a closer look into the eye and identifying them as “drusen”, small yellow dots. Prolonged or extensive drusen formation results in the death of retinal pigment epithelial cells in patches, producing bare spots commonly known as “geographic atrophy”.
What are the types of age related macular degeneration?
AMD or ARMD can be broadly categorized into two types:
i) Dry (Non-Neovascular) AMD
Once retinal pigment epithelium (REP) loses its support functions, the photoreceptor cells overlaying the geographic atrophy regions lose their function too, resulting in vision loss from that particular patch of the retina. A person can be classified as “legally blind” when these patches continue to grow, covering the “fovea” (the central most part of the macula), drastically reducing their visual acuity. This atrophic phase of AMD is also referred as “Dry Macular generation” or “Non-Neovascular AMD”.

Despite being the most common type of macular degeneration responsible for about 90% of the total AMD instances, Dry AMD generally progresses very slowly, identifiable in three different stages, i.e. early, intermediate and advanced.
In the earliest stage of Dry AMD, your eye gets drusen with normal vision, characterized by mild vision loss. When it advances, the area of central vision loss grows with increased probability of additional drusen and pigmentary changes. Though dry AMD conditions progress, they rarely advance to the level of legal blindness. However, this progression may result in macular tissue atrophy and mild scarring.
ii) Wet (Neovascular) AMD
Sometimes, the growth of choroidal blood vessels occurs within the retinal pigment epithelium and retina of people suffering from macular degeneration (apparently, as a result of your eye’s natural tendency to heal any defects in these layers) as a result of any injury to the RPE.
In fact, such a reparative process resembles to the formation of scars after skin abrasion anywhere else on skin. Since retina comprises of highly complex as well as sensitive tissues, the in-growth of these newly formed choroidal blood results in more visual loss as compared to the original degenerative process itself.

Ironically, wet AMD’s contribution in total number of macular degeneration cases reported doesn’t go past 10%, but majority of the legal blindness incidents are caused by this complication of macular degeneration.
When the dry form of AMD progresses to the wet form, new blood vessels are produced (the process also referred to as neovascularization) underneath the retina. These newly grown vessels are quite frail in nature, which can result in leakage of blood and fluid, often leading to lifting of the macula and visual distortions likely to damage tissues retina tissues permanently. Significant vision loss caused by scarring may also occur, going all the way to legal blindness.
Some other variations of macular degeneration include:
iii) Geographic Macular Degeneration
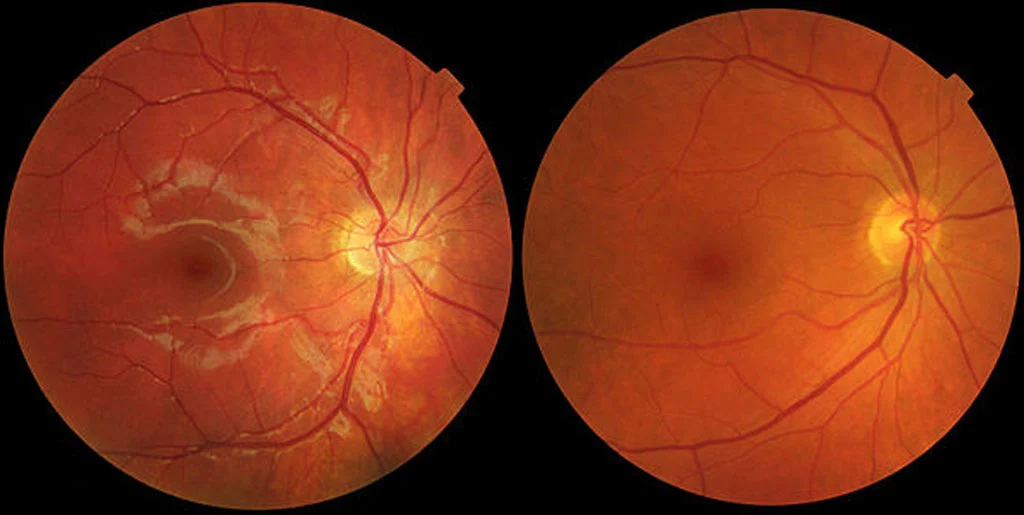
Geographic macular degeneration is considered as an advanced stage of dry macular degeneration, which is characterized generally with a large area that has lost its retinal pigment epithelial cells (RPE). The characteristic red-orange color observed at the back of the eye is courtesy to RPE cells, which is helpful in nourishment of the photoreceptors cells of the eye comprising of the rods and cones. That is why these rods and cones of the retina are eventually affected by any disease affecting the RPE.
Since the large areas of the RPE lost to macular degeneration are mostly surrounded by a sea of a healthy retina, the condition is referred to as “geographic atrophy”, sometimes also termed as “RPE dropout”. Generally, no significant bleeding or fluid leakage is observed under the influence of geographic atrophy, the loss of vision occurring quite slowly.
iv) Juvenile Macular Degeneration

Also known as “Juvenile Macular Dystrophy”, this particular variation of macular degeneration is inherited, affecting children and young people specifically. Mostly, this is an autosomal recessive condition, i.e. it develops only when a recessive gene is passed on to the child from each parent. This condition targets only the central vision in children, sparing the peripheral vision and the victims do not go blind by it. Juvenile macular degeneration is further bifurcated into two subcategories, i.e. Stargardt’s disease and Vitelliform macular dystrophy.
a) Stargardt’s Disease
Of the rare instances of macular degeneration in children and teenagers, Stargardt’s disease is the most common cause. The disease is named so after the German ophthalmologist, Karl Stargardt, who reported of the first ever case of this disease back in 1901.
Mostly, this eye disease develops anytime between the ages of 6 years to 20 years and affects both eyes.
The cause of this disease, just like its treatment, is different compared to commonly known types of age related macular degeneration. A gene known as ABCA4 is responsible for Stargardt’s disease, which is usually a recessive trait. There is a 25% probability of Stargardt’s disease affecting a child when both of the parents are carriers of the ABCA4 gene mutation.
Due to ABCA4 gene mutation, the normal transportation of food and waste material to and from the retina’s photoreceptor cells is blocked due to production of a special type of protein. Retinal Pigment Epithelium (RPE) is the layer responsible for nutritional support in the rods and cones of the retina, where waste deposits, the flecks of lipofuscin, start to build up as a result of this. Piling up of this waste starts breaking up the RPE, rods and cones within the retina.

Quite like other forms of macular degeneration, Stargardt’s disease also lacks a cure until now. Sometimes, if leakage of blood vessels (like in “wet age related macular degeneration”) is observed, intraocular injections of anti-VEGF drugs are used to treat it.
Mostly, appropriate nutrition and eye protection (particularly, sunglasses capable of blocking UV A & B and blue lights) helps in delaying the progression of the disease. Once vision begins to deteriorate, whether in the childhood, teens or twenties, resorting to low vision aids is the best way to go, helping to maximize the undisturbed peripheral vision.
It is important to consult a seasoned optometrist to seek advice on nutrition as soon as possible when suffering from Stargardt’s disease, because excessive amounts of Vitamin A, which are normally considered healthy food for eyes, can be really bad in this case, as it cannot be metabolized properly by the cells in the eye.
b) Vitelliform Macular Dystrophy (Best’s disease)
Vitelliform macular dystrophy, a genetic eye disorder also known as Best’s Disease, can lead to progressive vision loss, affecting the RPE (retinal pigment epithelium) underlying the photoreceptors (the light sensitive cells) of the macula inside the eye. Vision loss caused by Best’s disease can be variable, targeting central vision in one or both eyes.
Lipofuscin (a fatty yellow pigment) might build up in RPE from Vitelliform macular dystrophy, forming an egg yolk looking lesion (in fact, Vitelliform translates as “looking like an egg”). With the passage of time, cells critically needed for clear central vision can be damaged due to such abnormal accumulation of lipofuscin. That is why people suffering from this eye disease often get blurry or distorted vision, or even the total loss of central vision. However, this form of macular dystrophy typically spares peripheral vision, leaving the ability to see sideways and night vision unharmed.
Vitelliform macular dystrophy exists in two forms with almost similar features. The early onset form is commonly referred as the Best’s disease (named after the scientist who identified and reported the first case of this disease in 1905, Franz Best). It usually targets the vision of patients in early childhood, the symptoms and severity of the resulting vision loss varying significantly. The adult onset form generally commencing through mid-adulthood with a relatively mild loss of vision that progresses with the passage of time.
Vitelliform macular dystrophy, in each of its two forms, features signature changes within the macula, which can be detected through an eye examination. For instance, electo-oculogram tests can be a part of the examination for identification of this disease, whereby the electrical responses of the retina are observed after getting stimulated by light.
Currently, no effective treatment exists for Vitelliform macular dystrophy, though traditional as well as genetic scientific research on the subject may shortly lead to some successful treatments in future.
During the advance stages of the disease, formation of new, leaky blood vessels underneath the retina may occur in many patients (a process known as neovascularization, similar to what happens in wet age-related macular degeneration), which can also lead to central vision loss. However, under such circumstances, anti-VEGF drug-based injections into the eyes can now be used quite conveniently. This treatment works best when applied soon after new blood vessels are formed. So, patients of Vitelliform macular dystrophy are advised to self-monitor any changes in their vision with the help of Amsler grid.
This can help them observe any sudden changes while viewing the grid (for example, blurriness, distortion or any blank patches). In such a scenario, immediately consult an optometrist or ophthalmologist, as these can be the signs of neovascularization and the sooner it gets addressed, the higher would be your chances of slowing down the progression of the disease.
There is no significant evidence directly correlating the progression of vitelliform macular dystrophy with, but incorporating eye-healthy diet recommended commonly for age related macular degeneration into your daily routine can only be beneficial, to say the least. For instance, you can start consuming fish twice to thrice a week, prefer low GI (Glycemic Index) carbohydrates over high GI foods, and eat leafy greens daily with other fruits and vegetables, also adding a handful of nuts a week.
What causes macular degeneration?
Macular degeneration has been the subject of interest for scientists for well over a century by now. When they first observed drusen in the eye, using ophthalmoscopes in late 1800s, they considered it infection or inflammation of some kind, of the choroid. In fact, even to this day, some evidence suggests that somehow body’s own immune system has some role in the development of some forms of macular degeneration, the neovascularization in particular.
i) Environmental Factors
Environmental factors are also considered as another group of probable causes behind macular degeneration. Epidemiologists have been exploring this area for a long time and some of the factors studied by them so far include nutritional factors (like antioxidants, zinc, and B-vitamins), drugs, (like nicotine, caffeine, and oral contraceptives), various types of toxins as well as light exposure. Though some of these factors have exhibited reasonable effect on the prevalence of macular degeneration (i.e. leafy vegetables help against the progress of the disease, while cigarettes are known to contribute to its progression), none can be considered as the likely major cause behind it.
ii) Genetic Factors
Mild genetic abnormalities constitute another group of probable causes of AMD. Some forms of macular degeneration have been known to run in families for over a century. For about last 25 years, an increasing body of evidence has been collected that considers heredity a significant factor in prevalence of age related macular degeneration.
This has also served as a considerable assistance in understanding AMD at the molecular level, which has been helpful in development of enhanced treatments for the disease. Identification of a dominant gene group as the major cause of age related macular degeneration in a person means higher probability of other family members being affected by the disease in the same manner. Modern day molecular genetic methods can then be used to further study such families to pinpoint the causative gene.
One of the major appeals of this type of genetic approach is identifying a genetic predisposition to AMD, which means increased possibility of testing for the predisposition for the affected individuals earlier in life, offering some treatment capable of delaying or preventing the onset of macular degeneration. Such treatment(s) is more likely to be safer and cheaper (thus more readily available) compared to other experimental treatments under consideration currently.
What are some of the signs and symptoms of age related macular degeneration?
Regions of atrophic retina might be visible to an ophthalmologist in the macula in both dry and wet forms of AMD. However, fluid or exudative material within (or under) the retina might only be observed in wet forms of the disease.
Macular degeneration is basically a painless condition with no visible symptoms in most cases until the disease has already progressed to advance stages.
Dry AMD Symptoms:
There might not be any noticeable symptoms related to Dry AMD for up to about 10 years after its onset, taking even longer in appearing if only one eye is affected. Those that appear may include:
- Problems reading under low light conditions
- Blurriness setting in reading printed or written texts
- Problems adjusting to exposure of bright light
- Inability to see the vibrancy of colors like before
- Problems recognizing people’s faces
- Losing sharpness of the vision
Wet AMD Symptoms
Wet AMD symptoms may comprise of any or all of the above symptoms, and the following ones additionally:
-
Metamorphosia – a condition in which a person sees straight lines as crooked or wavy
-
Central Scotoma – Appearance of a blind spot in the central vision, which continues to grow if left untreated
It is highly recommended to consult an optometrist or ophthalmologist as soon as you notice any of the above mentioned symptoms, because early diagnosis and timely treatment can improve your odds against vision.
What are the stages of age related macular degeneration?
There are three stage of AMD:
i) Early AMD
Vision loss doesn’t set in for most people through the early stage of AMD, which is what makes regular eye exams so pertinent, especially if you are among people having more than one risk factors of the disease. Presence of medium-sized drusen (yellow colored waste deposits found beneath the retina) helps optometrists diagnose early AMD.
ii) Intermediate AMD
There might be some vision loss by this stage, but still most likely to have no noticeable AMD symptoms. You will need a comprehensive eye exam from an optometrist/ophthalmologist aimed at finding larger drusen and/or changed pigmentation of the retina.
iii) Late AMD
Vision loss becomes noticeable at this stage.
According to National Eye Institute (NEI):
What are the risk factors for age related macular degeneration?

Risk factors for AMD include:
i) Smoking: According to research, smokers are two to three times more likely to develop age related macular degeneration compared to their nonsmoking peers.
ii) Diet: Dietary intake has been known to affect the progression of AMD for a long time. For example, a diet loaded with highly processed and packaged food devoid of fresh vegetables can contribute in rapid progression of age related macular degeneration.
iii) Obesity: Studies reveal that the risk of developing advanced AMD is doubled when you are obese.
iv) Hypertension: According to studies conducted by the National Eye Institute (NEI), the probability of developing wet AMD increases by 1.5 times in people suffering from hypertension.
v) Sunlight Exposure: Though lacking in conclusive evidence, long term sunlight exposure is believed to contribute in progression of AMD due to harmful effects of UV (ultraviolet) light on retina.
Above mentioned risk factors for AMD are considered to be controllable, while the risk factors for age related macular degeneration beyond our control are listed below:
vi) Age: Age, without any doubt, can be considered the greatest risk factor for AMD. Although macular degeneration might strike someone during middle age, people over 75 years of age are the likeliest to be victims of AMD, in fact 30% more than people below 60 years
vii) Gender: Yes, gender is also believed to play a part beyond our control in age related macular degeneration, females having higher likelihood of becoming the victims.
viii) Race: Race, like gender, also plays a role in development and progress of AMD. According to studies, Caucasians are more likeable targets of AMD in the U.S. as compared to African-Americans.
ix) Iris Color: Eye color, courtesy to the color of pigments within the iris, also matters in determining your chances of developing age related macular degeneration, i.e. people with light-colored eyes are more probable to become victims of dry AMD.
x) Genetics and Family History: Heredity doesn’t account for all types of macular degeneration, but scientists have been able to identify certain genes capable of determining a person’s risk of developing AMD. Similarly, a person with a parent, siblings or other close family members is three to four times more likely to be affected with AMD.
Who can treat macular degeneration?
An optometrist or ophthalmologist is the right person to diagnose and treat you for macular degeneration. An ophthalmologist is a full time medical doctor with years of specialized training in diagnosing and treating eye diseases medically as well as surgically.
The diagnosis of macular degeneration involves dilation of pupils using eye-drops, which enables the ophthalmologist/optometrist to clearly see the retina. Once AMD is diagnosed, they determine whether it is the dry macular degeneration or the wet type.
If a non-ophthalmologist diagnoses your macular degeneration, he might refer you to an ophthalmologist specializing in the treatment of vitreo-retinal diseases.
Diagnosis of Age Related Macular Degeneration
Though age related macular degeneration is asymptomatic in its early stages, sometimes patients experience certain symptoms like acute vision loss, blurred vision, scotomas, metamorphopsia, chronic visual distortion and so forth.
However, no significant symptoms are observed in AMD/ARMD patients in majority of cases, which is why experts recommend you to take detailed eye examinations at regular intervals.
In fact, primary care physicians shall be aware of their patient’s overall health profile to successfully identify and recommend AMD high-risk patients to the ophthalmologists, who can then go ahead with appropriate diagnosis.
Any reliable ophthalmologist doesn’t establish his final diagnosis without taking a few critical tests, which include:
Amsler Grid: This test requires the patient to have a look at a specially designed grid comprised of horizontal and vertical lines. If a person is afflicted with age related macular degeneration, seeing the grid in its original formation is not possible, it will appear to be faded, broken or distorted at places. In fact, the results of viewing the grid help ophthalmologists gauge the degree of damage done to the eye. To majority of people with detectable symptoms of AMD, the lines constituting the centre of the grid appear as broken, faded or distorted.Fluorescein Angiography: This is the test used to confirm the type of AMD afflicting a person, usually required to be taken after the suspicion of wet AMD. Eye doctor examines the eye of the patient using a specially designed magnifying device after injecting a special type of dye into the patient’s arm. This is followed by a series of the examined eye’s pictures, which helps the eye specialist determine whether or not the blood vessels underneath the macula are leaking. Any leakage in the blood vessels confirms the case of wet AMD.
Optical Coherence Tomography (OCT): In this method, the optometrist collects additional data about the macula by seeing the image of a retina scan taken using special light rays. The image reveals whether the macula has undergone any changes, i.e. gone thicker or thinner than it is supposed to be.
What are some important questions that you should ask your eye doctor?
One of the best ways to know about the condition of your eyes, the diagnosis and possible treatment, is to ask your eye doctor about them until you develop a clear understanding about them. Some of the most critical questions to ask might include:
- What’s your diagnosis of my eye(s) condition? Please spell out the medical terminology used for it.
- Is my case of age related macular degeneration treatable?
- How is this condition going to affect my vision right now and in future?
- Are there any particular symptoms that I should watch for and how to intimate you if I observe any of them?
- Are there any lifestyle changes that can help me better cope with my AMD?
Prevention
Increasing age of the population also means increased risk and impact of age related macular degeneration in the future, which makes it imperative to look for better preventive strategies and improved treatment options. That is why experts consider identifying and attacking ARMD in its early stages to slow down the progression of the disease and vision loss as one of the best strategies. Lifestyle changes, including dietary constituents, have been proven quite beneficial in preventing the progression of AMD and you can find a detailed account of all such elements in this write-up.
Age Related Macular Degeneration Treatment
A handful of treatments exist for macular degeneration, also referred commonly as age-related macular degeneration (AMD/ARMD) – an eye condition resulting in gradual demise of the central vision. However, almost all of these treatments merely prevent or slow down the damage to the retina. Unfortunately, they are not able to repair the already damaged regions of the macula, or restore the vision lost due to that. Depending upon the extent of the damage done to your eye, various vitamins, medications, therapies and surgery can be subscribed to you by your eye doctor. Moreover, wet and dry forms of AMD are treated distinctively.
What is the treatment for wet macular degeneration (Wet AMD)?
Three different approaches are used to treat wet AMD, i.e. laser surgery, photodynamic therapy as well as injections into the eye, none of them considered as a permanent cure of the disease though. Progression of the disease and loss of vision may continue despite treatment.
i) Laser Surgery for Wet AMD
In this type of treatment, fragile leaky blood vessels are destroyed with the help of laser surgery as photocoagulation. A high-energy light beam is focused directly onto the growth areas of newly formed blood vessels, annihilating them to prevent any further vision loss. However, there is a downside to this treatment. The probability of destroying some healthy tissues surrounding the clusters of newly forming fragile blood vessels cannot be ruled out completely, which can cause further loss of vision. That is why experts recommend this treatment only for patients who have the growth of new vessels away from fovea, the very central region of the macula. There is only a limited fraction of the total number of people suffering from AMD who can actually take advantage of this type of treatment for wet AMD. Even in the people treated with laser surgery for wet AMD, there is a significant probability of re-growth of new blood vessels, again requiring surgery or some other type of treatment.
ii) Photodynamic Therapy for wet AMD
A drug known as verteporfin (Visudyne) plays a vital role in photodynamic therapy for wet AMD. The doctor injects the drug into a vein of the arm. Then, the diseased eye is exposed to a light of a specific wavelength, so that the drug can be activated to destroy the newly formed blood vessels, slowing down the rate of vision loss ultimately. Unfortunately, this treatment also remains unable to completely stop the loss of vision or restore any of it already damaged by this advanced form of macular degeneration. The results of photodynamic therapy often remain temporary, requiring retreatment in many cases.
iii) Anti-VEGF Therapy
There’s one avenue that has undergone significant progression in last decade or so with respect to the treatment of wet macular degeneration, i.e. injections of specifically developed drugs into the eye aimed at halting the escalation of new blood vessels. Research has already shown that new blood vessels need a specific type of chemical for their growth under the retina, known as “Vascular Endothelial Growth Factor” (VEGF). Since the drugs used in these eye-injections are meant to counter the growth of new blood vessels in the retina, the treatment is also referred as “anti-VEGF pharmacotherapy”. In fact, cases of regression of the damaged retina have also been reported as a result of injecting VEGF drugs into wet-AMD affected eyes. The VEGF drugs used for treating wet AMD include:
- Eylea (Aflibercept) – FDA approved
- Lucentis (Ranibizumab) – FDA approved
- Avastin (Bevacizumab) – Not approved by FDA for AMD treatment
Whereas Eylea and Lucentis are approved by the FDA for treating people with wet AMD conditions, Avastin still remains unapproved for such treatment (though it is approved for the treatment of colon and other types of cancers). Injecting Avastin into the eye requires compounding under highly professional supervision and some physicians resorting to it only do so because of its considerably lower costs. For treatment of wet AMD, these drugs need to be administered directly into the vitreous of the eye only by a qualified and experienced ophthalmologist, mostly on a monthly basis. Once administered, the eye needs to be monitored comprehensively to determine the effects on the eye, on a monthly basis for Lucentis and every other month for Eylea.
Anti-VEGF injections’ treatment is known to halt or slow down vision loss significantly in a considerable number of patients, some even experiencing a certain degree of improvement in their vision. In fact, VEGF inhibitors are being adopted much more frequently nowadays compared to laser ablation as well as photodynamic therapy. With newer, constantly improving VEGF inhibitors currently running through clinical trials (also including drugs specifically developed to counter platelet-derived growth factors as well as angiopoietins) and ready to approach the market, a patient’s odds of a better outcome are significantly boosted if this type of macular degeneration is diagnosed and treated early on.
What is the treatment for dry macular degeneration (W AMD)?
Of all treatments available for dry macular degeneration currently, none is able to completely reverse dry AMD. However, this particular disease of the eye progresses relatively slow and most patients are able to live their lives quite actively and productively despite having this eye condition.
AREDS and AREDS2 based Dry AMD Treatment
There is no treatment that can prevent further vision loss once dry AMD progresses to a significantly advanced stage. However, the progression of intermediate AMD to advanced AMD can be seriously delayed (or even prevented in many cases) by taking a combination of medications based on the AREDS and AREDS2 studies conducted by “The National Eye Institute’s Age-Related Eye Disease Study”.
These studies revealed that a specifically designed high dose of selective antioxidants and zinc was able to significantly counter the risks of progression of intermediate-stage dry AMD to advanced stage. This proves equally effective in subduing the progression of visual loss in many people.
The antioxidant formulation used in these studies comprised of vitamins C and E, beta carotene (vitamin A) and zinc. These studies were not able to produce viable evidence to suggest that this formulation offers any solid relief to people suffering from early-stage dry AMD. However, it works well enough for people having intermediate-stage macular degeneration in one or both eyes or any form of advanced AMD (wet or dry) in only one but not the other eye. As a precautionary measure, people with an increased risk of lung cancer better avoid taking beta-carotene. Currently, more studies are underway on supplements including zeaxanthin, lutein, some other carotenoids, bilberry and black currant to find even better protection against dry AMD.
Coping with Macular Degeneration
Though macular degeneration mostly spares your peripheral or side vision, it is known to affect central vision without leading to total blindness, making it difficult to perform daily-life activities like recognizing people’s faces, reading, writing, driving and other activities requiring sharp central vision.
This can be much of a startling experience, but the key to overcome such a significant ordeal is to embrace your condition and learn to live well with AMD. One of the best ways to commence on your journey of living well with age related macular degeneration is to seek help from low vision centers. They have the capabilities of assessing your low vision conditions, suggesting different optical and household devices to make up for your near-vision tasks. You can also ask your eye doctor about the nearest low vision centers in your vicinity.
Some simple but effective ways of coping with macular degeneration include:
Travel with caution: Driving should be the very first thing to take extra care of when suffering from low vision conditions due to age related macular degeneration. Immediately consult with your eye doctor, so that he can assess your ability to drive safely based on your current visual acuity. Make sure to avoid certain situation while driving, such as driving at night, driving through heavy traffic or bad weather conditions. It is even more advisable to ask your family members for help and preferring public transport over driving, especially during the night.
Grab a pair of appropriate glasses: An appropriate pair of glasses can help you make the best of the vision you are left with, having an extra pair in your car is even better.
Prefer reading large prints and fonts: If you are fond of reading, you can still continue to do so despite your low vision conditions by resorting to books and magazines with large prints. Similarly, you can also surf through internet with websites featuring large fonts and offering to alter the font size according to your preferences.
Look for specialized appliances: Specialized appliances also help people with low vision conditions; for instance, clocks, telephones and other such appliances with extra-large numbers and digits.
Learn to light up your home rightly: Reorganizing your lighting fixtures is another way to ease your life when low vision issues start bothering you. Lighting up your home rightly can help you with reading, finding your desired stuff conveniently, and so forth.
Furnish rightly: Similarly, you can refurnish or reorganize your existing furniture according to your habits, needs and requirements, steering clear your pathways to make sure your movement remains smooth and safe.
Reach out to your family and friends for help: Don’t feel shy in approaching your family and friends for help. Share your problems and concerns with them and you will be amazed to see how cooperative they can be in helping you perform different tasks conveniently.
Don’t isolate yourself socially: One of the biggest issues people suffering from macular degeneration come across is the inability to recognize faces and remember names, which leads many of them to social isolation, unfortunately. This is like accepting defeat at the hands of your illness and can lead to severe depression. The best way is to embrace your condition, share your problem with people you have to meet and greet, and ask them to tell you their names. You will be surprised to see how willing and helpful people can be once you reach out to them the right way instead of confining yourself to your home.
**Find likeminded people and groups:**Having likeminded people to share your views, ideas and concerns is always a relief. The good thing is that more and more people are getting aware of the graveness of macular degeneration and you can find many support groups online. Join them and learn to live newer, better and innovative ways of living the best you can with macular degeneration as a part of your life.
Resort to low vision aids: Thanks to rapidly advancing technology, specially designed low vision aids for macular degeneration like “Iris Vision” are available nowadays, which enhance the quality of vision amazingly well for people suffering from AMD, cataracts, glaucoma, and various other eye problems.
To conclude, remember, nothing is stronger than your will to fight through an ordeal. So, if you are willing to live a successful and thriving life despite being a victim of macular degeneration, nothing can stop you in doing so.